1000 Days Project
Posted by markdlevy@gmail.com on Dec 14, 2012 in Blog | 0 commentsThe 1000 Days Initiative is a transformational program for developing healthy mothers and thriving babies amongst economically vulnerable populations. It is an integrated approach offering wellness and health services over the course of a woman’s pregnancy and the first two years of her infant’s life. It combines best practices for maternal and newborn care in a single, unified package.
The 1000 Days Initiative:
Transforming Maternal and Child Health and Wellness
Prepared by:
Public Health Foundation of India
Apollo Hospitals
Ashoka Health for All
Harvard School of Public Health
Introduction
Solutions for saving and improving the lives of childbearing women and their children are failing to achieve the Millennium Development Goals established by the international community. Disconnected interventions, failure to implement known best practices, over emphasis on acute care, and the high costs of traditional doctor and facility-based medicine are endemic barriers. We need to build an effective system for maternal, newborn, and child health (MNCH) that integrates successful interventions, ensures delivery while improving quality, covers the full continuum of care, strengthens health systems while reducing cost, and is sustainable. And, mothers and babies deserve care that goes beyond simply aiming to prevent death or injury, but instead helps create healthy families that can achieve their full human capacity.
The 1000 Days Initiative is a transformational program for developing healthy mothers and thriving babies amongst economically vulnerable populations. It is an integrated approach offering wellness and health services over the course of a woman’s pregnancy and the first two years of her infant’s life. It combines best practices for maternal and newborn care with proper nutrition and breastfeeding, immunization, and clean water interventions in a single, unified package, delivered primarily by village health workers operating from local wellness centers — and makes sure those happen and can be measured in real time. This is possible by leveraging proven components of information technology, services, and research methods and combining them to create a novel, holistic and scalable system of distributed health that invokes facilities-based medical care only when it is needed. The Initiative will combine the capacities of leading public and private organizations to create sustainable, replicable, and outcomes-oriented synergies, using widely accepted interventions, enabled by the latest wireless information and communications technology (ICT).
Our initial goal is to create a test bed of over 1.5 million people in India (with a parallel program in Bangladesh) who will be provided this integrated service package, using three different business models — government, NGO, and private pay – backed up by a world class research program. We aim to reduce maternal and newborn mortality by approximately twenty five percent. We also seek to halve the prevalence of maternal anemia and stunting and to reduce the overall disease burden. But far more than merely reducing disease and mortality, our critical goal is to yield substantially improved wellness outcomes so we can generate and sustain consumer demand for a system of wellness and health care. Consumer demand is critical to the behavior changes that are needed for transformative changes.
Creating this wellness model for rural areas has multiple implications for implementing countries, including increased worker productivity, mental and physical capacity in the next generation, and significant future savings in health costs and disease prevention. The Initiative expects to advance the health and prosperity of poor communities in the developing world by empowering a generation of mothers and infants, and to demonstrate the effectiveness of an integrated, ICT-enabled approach in achieving these goals. We also anticipate that the system implemented will serve as a new model for primary health care delivery that can be implemented in flexible ways around the world.
Why This Initiative is Unique
There is relatively universal agreement on the individual interventions necessary during the 1000 days period to address the most common causes of mortality and morbidity for mothers and infants. Indeed, across the world, large numbers of programs are underway that include select elements of the required services. These are generally separate programs, ranging from efforts to arrange emergency care, to educating expectant mothers on the value of breast feeding, to child immunization programs, to providing clean water.
There are also many examples of pilots around the world using modern ICT to support specific health interventions, including during the 1000 Days period. There is, to our knowledge, no example where all four major intervention groups have been combined into a single initiative, extended over the entire “continuum of care”, and supported by a single ICT system with a strong mHealth focus that is interoperably connected to the doctors and hospitals of an excellent traditional health system.
We plan to combine the consensus high impact interventions during the 1000 Days into a single, integrated package focused on the twin goals of safe birthing and the launching of healthy babies who are able to achieve their full potential in life. The Initiative’s services will be focused at the community and household level, and will be delivered through a system that is both horizontally (multiple interventions throughout the 1000 day continuum of care) and vertically integrated (from household and health worker up to acute care when it is needed). We will register families to participate, opening individual electronic health records, and getting commitments from them to commit fully (i.e. drink clean water, eat the nutrition supplements, attend checkups) in return for access to the benefits of the program.
By linking all these together in a single program with a single information system, we believe we can lower costs, improve delivery and accountability, and develop attractive packages of services that the public will want. In addition, our leveraging of mobile technologies as part of an overall, integrated system will yield multiple benefits. These include: providing a wide variety of information to the public; enabling the provision of services by staff with less formal training; improving training and effectiveness of supervisors; reducing the reporting burden while vastly improving data collection and flow; addressing quality and accountability through standardization and the use of electronic protocols; ensuring effective patient follow up; and integrating the services of different organizations.
We also intend to test the sharing of centralized support functions over multiple field service activities. These shared functions include but are not limited to: call center (or center systems), telemedical consultations, research, and training content.
We are actively recruiting additional sponsors and partners from other fields that will play roles in the eco-system needed to deliver this transformed approach (especially IT, communications, consumer products, pharmaceuticals, finance, and insurance.) Our goal is to use the Initiative to find hybrid, shared value business models that are sustainable while being accessible, delivering the different returns the various parties need.
The following is a simple eco-system diagram. Beyond public health and wellness outcomes, one of the critical goals of the Initiative is to begin to understand the new forms of public and private relationships between the functions in this organizational eco-system diagram.
We also anticipate that the ecosystem we are establishing through the 1000 Days intervention will lend itself to the identification and initiation of related social enterprises. Setting up a sustainable ecosystem will allow other participants to engage that system and identify and develop programs that respond to unmet. For example, if this kind of system existed, one can imagine an entrepreneur establishing a rural blood bank as a new “node on the network.”
The entire system is designed to keep communities healthier, starting with mothers and babies, in a highly effective way at low cost. Key factors that we believe will lower costs, allowing services to become increasingly available and affordable, include:
- Reducing the initial disease burden and, thus, the demand for expensive critical care
- Providing care where people live, saving them money in travel costs and lost wages
- Using science-driven protocols to improve quality and efficiency of care
- Enabling frontline health workers to provide wellness and health services in a distributed health system, and thus limiting use of expensive assets like doctors and hospitals to when they are needed.
Maternal and Child Health Services
The four critical wellness, prevention and care areas the Initiative will address are outlined in the chart below. The package is designed to both enhance well-being, and reduce the need for more expensive and acute services:
| Maternal and Newborn Care | Nutrition | Immunizations | Clean Water Services |
| Sign up for package; educate woman and her key family members | Record nutritional status | Use as electronic shot record and reminder | Sign up for water package |
| Create electronic health record for mother and then baby; regular appointments with OB/GYN, nurse | Educate woman and her key family members | Educate woman and her key family members | Educate woman and her key family members |
| Key diagnostic tests for mother and baby (HIV, high blood pressure, GB strep, gestational diabetes, anemia, syphilis, fetal ultrasound, etc.) | Test for nutrient repleteness at regular times during and after pregnancy (glucose, hemoglobin/iron, protein, etc.) | Provide reminders of immunization schedule and support government drives | Record water use |
| Warning signs of problems-(vaginal bleeding, severe stomach cramping, lack of fetal movement, etc.)Referrals for acute care as necessary | Dietary education and instructions for pregnant women | Collaborate with government to administer shots for pregnant women (Tetanus Toxoid) | Monthly clean water package provided |
| WHO/Gawande birthing checklists; provide misoprostol; seven day after birth checklists | Education and encouragement for pregnancy nutrition and exclusive breastfeeding for 6 months and until age two | Promote public education and encouragement for vaccinations | Sufficient water for drinking, which supports breastfeeding |
| WHO Integrated Management of Childhood Illnesses; referrals to acute care as necessary | Delivery of bio-available nutrient supplements for pregnant women and babies 6-24 months to ensure nutrient repleteness (including folic acid, iron, Vitamin A, others) | Support and record govt immunizations for newborns and infants (DtP, Pneumococcal, Polio, Hib, MMR, Rotavirus, Hepatitis A, B, etc.) | Water provided for all family for drinking and cooking |
Delivery System
A key element of the model’s delivery system is mobile health workers. They engage the community to raise awareness, sign mothers up for the “1000 Day” pregnancy and newborn service package, conduct monthly home checkups, and offer education and guidance to mothers and fathers regarding healthy pregnancy, labor and delivery, and infant care and feeding. They are the “wellness marketing and patient education” staff, with a full array of scripts to follow, explanatory videos to show, and answers to common questions, all housed on an electronic tablet. They also provide treatment follow-up and compliance monitoring, and bring information gathering, screening tools and even case management to the doorstep. A central focus of the Initiative is to empower them with modern information tools.
These workers are based out of community wellness centers that provide the clean water, nutrition, diagnostics, and public education materials, including access to online resources. The centers are the meeting place for group and individual sessions (4 times per pregnancy) with a traveling OB/GYN, nurse and paramedic, carrying the latest in remote diagnostic and monitoring devices. This approach resembles the “camp” model with which people in rural India are familiar and will be replicated four times a year for new babies. These contacts will be backed up with a clearly defined system for referrals to doctors and hospitals for acute and emergency care as needed. In addition, the Initiative includes a detailed examination of the use of telemedical access, and call and information centers to provide answers to the public and front line providers. The Initiative will undertake a variety of experiments with these concepts to determine the most effective and efficient uses of them.
The field workers and call center will provide real-time triage/referral to doctors, specialists and hospitals. This health worker-wellness center-telemedical center system provides novel synergies and serves multiple purposes, both extending primary care to people’s doorsteps and using scarce and expensive resources from the traditional medical system only when needed. In each area where we will operate there are traditional medical clinics and hospitals. We will engage those providers so they are prepared for referrals, and understand the benefits we will be providing to them. The medical experts at Apollo will provide overall health supervision.
Information and Communications Technologies
Every link in this chain is enabled by the latest in modern, mobile ICT. We know that wireless technologies are rapidly becoming a reliable communications infrastructure in rural areas of developing countries. We also know that “smart” mobile devices with the capacity to support advanced tools for mobile workers are now becoming affordable. For example, $100 wireless Android tablets are becoming available in India this year. With appropriate content and backup systems and people, such devices can compensate for the lack of medically-staffed rural frontline facilities. They can enable community health workers with modest training to become the leading edge of a transformed healthcare system. Indeed, by providing the backbone for assurance that medically defined protocols are being followed, we believe quality can be improved.
Rather than inventing new mHealth software, we will use and connect best-in-class products that have been proven in the field. For example, each community health worker will be provided with a tablet that includes an upgraded and expanded version of Dimagi’s CommCare, a maternal health software package with relevant checklists and other electronic protocols. We will also utilize the MAMA Initiative’s mobile health information services to provide expectant and new mothers (and their families) with useful health information and advice through their cell phones. The cloud-based ICT system provides access to sophisticated decision-support tools for wellness center and mobile health workers, and automated message delivery to patients (e.g. weekly voice calls and/or text messages for pregnant woman).
The ICT systems will also help encourage and track the public’s engagement with the program’s services. Every woman of childbearing age will be registered and given a secure electronic health record (EHR) for herself and her newborn that is shareable across the continuum of care and with the traditional healthcare system when it is invoked. Health providers will be able to enter and access patient data through medical algorithm-driven software using a mobile tablet or computer.[2] Standardized checklists will be used to track and record a variety of important maternal and child wellness information in the EHR, including: family context; health status; vitals; pregnancy-related events; antenatal and postnatal visits, interventions; test results; labor and delivery; infant inoculation dates and requirements; and water and nutrition information. The community health worker and wellness centers/clinics will also be notified of automated risk categorizations, and supervisors will be told when visit data is delayed or missing. Nurses and doctors who are visiting the women physically or virtually will prioritize their work based on this information.
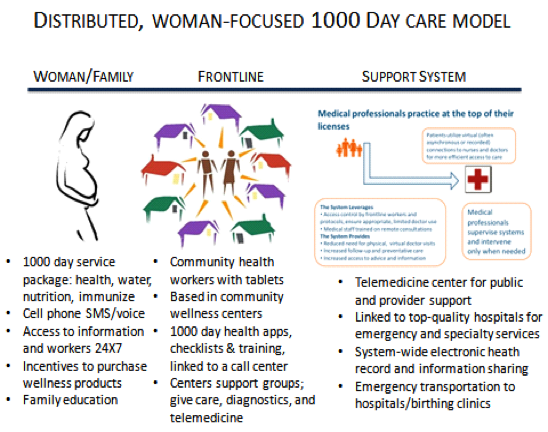
The following visuals demonstrate how ICT systems provide a variety of information and services across the continuum of care, integrating over time and vertically up to acute services when those are needed. They also enable task shifting of health care services as shown in the second diagram, freeing the doctors to focus on the problems that require their attention:
Training
Implementing the 1000 Days system will require new forms of training for the public and health care personnel – both in person and through electronic means. This training can educate and empower these groups, enabling women to take more responsibility to ensure the health of their family and allowing health care staff, particularly those with less training, to effectively and efficiently manage larger populations using ICTs.
Public education about the 1000 Days will be approached through “push” communications to women that emphasize health and wellness literacy. We will draw upon the vast amount of content developed globally for this purpose (such as by the MAMA Initiative), including radio, video, voice/message, and group approaches, and make appropriate modifications for local customs and languages. We will also provide women with access to health and wellness information, data bases and medical response centers. We will experiment with the most effective approaches to the latter.
A distributed wellness system requires different skill sets than traditional medicine, including:
| Role | Training Required |
| Village health workers | Gaining families’ trust, securing commitments from women/families. Using modern ICT to conduct monthly interviews. Identifying pregnancy/infant health danger signs. |
| Public health nurse/manager | Managing a series of health workers, and running the system out of a local wellness center over the 1000 Days of care, later becoming responsible for the overall wellness and health of a community. |
| Medical response center staff | Using electronic decision support protocols and patient’s EHR to effectively address patient and front line health provider questions/concerns and determine relevant actions needed. |
| Nurses and Doctors | Same as MRC staff, plus supervising physical and virtual medical response centers; using data to target people needing expert care. |
| Managers | Running the entire system, particularly to use the information gathering, data mining, and analysis tools they have access to. |
Formal training for integrated systems of this kind does not exist for the most part. The staff need to be instructed in the use of the new approaches and the electronic systems that support them; the training must continue over time and be available as “just in time”, or “point of care” training for specific circumstances. The program will use the ICT systems to enable, instruct, and measure providers in implementing the required services and interventions. As with public education content, we will utilize the best global content developed for this purpose and make proper adjustments for local contexts.
There is significant funding in the budget to develop formal in person and on-line/mobile courses and software to assist with both training and management of field staff. We will use the telemedicine links to the wellness centers for on-going staff training sessions, making efficient use of experts. Both PHFI and Apollo have extensive expertise in training and will be seeking best in class tools from around the world to use.
Business Model
As mentioned above, the program will be using three different business models — government, NGO, and private pay. We plan to coordinate with, learn from, and hopefully strengthen a number of innovative government programs, including mHealth ones (see, e.g. MCTS[3]). For the private pay approach, we will build on the successful eHealthpoint rural health and wellness model in Punjab, India, developed by Healthpoint Services. The program provides a network of clinics- each surrounded by 2-3 standalone water points in smaller neighboring communities. Each cluster (a clinic and its satellite water units) employs, in addition to its operating staff, several mobile health workers who visit families in their homes. Today these are walk-in clinics with pharmacies supported by a telemedical link to doctors for consultations.
These systems are currently cash flow positive, charging about $1.50 per month for an entire clean water supply for a family of four; $.80 for a telemedicine consultation with a doctor and less than $1 for most diagnostic tests. This will be expanded in the Punjab into the 1000 Day service package of maternal/child health, nutrition, water and immunization.
Apollo will test another version of this private pay model for this package around Aaragonda, in Andhra Pradesh.
For implementing the 1000 Day service package through a government model, we are in serious discussions with a highly respected quasi-governmental organization. It would trial the same system in a large area of northern India where it recently completed a highly successful test of the protocol for India’s Integrated Management of Childhood Illness (IMCI). The 1000 Day program would expand that service and provide strong ICT underpinnings to it.
In addition, we are in detailed discussions with several well-respected, local social enterprises and NGOs to provide the frontline service delivery in whole or in part through a subsidized model. They will utilize the components of the support system, such as the protocols, telemedical response center, ICT systems and support, and hospital medical support to save costs and ensure continuity of care.
Research
A key purpose of the 1000 Days Initiative is to find the optimum combination of parties, interventions, sources of revenue, and (where relevant to the business model) pricing — while sharing lessons, practices, and ICT tools so others can improve the efficiency and effectiveness of their programs. As a result, a significant budget for research, monitoring and evaluation is included. The Initiative will undertake a variety of research activities to ensure continuous improvement of its services, improve the sustainability of its business models, and to share and manage the knowledge that emerges from its efforts.
The research and evaluation program will be led by PHFI, with significant assistance by the Harvard School of Public Health and involvement from Apollo. Detailed control sites and methods, along with key metrics will be established. The Initiative’s monitoring and evaluation activities, fueled by the electronic health records data, will include the assessment of health and wellness outputs and outcomes, health system efficiencies, equity in health care service coverage, cost savings, and women’s empowerment, as measured through their decision-rights, health seeking behavior, and behavior change. A leading business management firm is being recruited to lead the study of the economics, business models, and outcomes of the overall eco-system and its component parts, with a particular focus on sustainability.
Creating a sustainable business model also depends on understanding how the beneficiaries react and respond to the package of services being provided. As a result, PHFI, Apollo Hospitals, Healthpoint Services, and the other implementation partners will conduct rigorous market research and feedback surveys of the target population. They will combine their understanding and experience to ensure that the real needs of the women and children being served are met in a culturally appropriate and impactful manner for each of the areas.
With respect to program improvement, the program’s vast ICT-enabled data will be utilized to improve execution, drive efficiencies, and subsequently achieve greater impact among the targeted population. In addition, over time the Initiative will be testing increasingly sophisticated decision support and device inputs, especially remote diagnostic and monitoring devices, to determine which are most effective.
In the area of knowledge management and sharing, PHFI will manage global expert advisory committees in five key areas: health and wellness, training (public and providers), ICT, outcomes research, and economics. They will ensure that our protocols and processes reflect global best practices. We also plan to develop a database to identify and map the relevant mHealth and eHealth activities in South Asia to ensure that the test bed is benefitting from the successes and/or failures from around the world, and that the Initiative is contributing its experiences. This will be coordinated with India’s new Health Portal, WHO and other international partners. In addition, the Founding Parties have become full sponsors of the “3rd International Conference on Transforming Healthcare with IT 2012”, which has been developed by Apollo Hospitals and will occur in Hyderabad, India on August 31 and September 1, 2012.
Budget
Phase one of the Initiative is designed to trial the delivery system. It will serve a population of 50,000 to 75,000 in Punjab and Andhra Pradesh. Deliverables will include the integrated protocol of the four services over 1000 days, supported by an ICT prototype that is deployed through a mix of new, existing, and upgraded wellness centers and their staff. The intervention package will be tested and refined based on the results and feedback from the communities we serve, including research of women’s preferences. The second phase will perfect the model, use the three different business models mentioned above, and expand to two additional areas of India, covering a total population of 1.5 million and including approximately 375,000 households. As the service population expands over the first three years, so will the number of wellness centers and public health personnel. A total of 62,000 pregnancies and infants will be addressed in the three year plan. The test bed we create will lend itself to additional operational and behavioral interventions. We intend for the test bed to be expanded and extended beyond the three years of this budget.
The Initiative’s budget includes expense categories for health and wellness, training, thought leadership and engagement, research, information and communications technologies, grants to implementing partners, and project staffing, management, and overhead.
Project Partners
Harnessing the power of public/private partnerships called for by United Nations’ Millennium Development Goal 8, the 1000 Days Initiative creates a first example of the complex eco-system required to sustainably deliver a transformed primary health care system. Each of the project’s four founding partners — Public Health Foundation of India, Apollo Hospitals, Ashoka Health for All, and the Harvard School of Public Health — will lend its unique expertise and strengths to the effort. Additional implementing and supporting partners are being recruited.
The Public Health Foundation of India (PHFI), sponsored by the Indian Government, the Bill and Melinda Gates Foundation, and private philanthropists, is the leading public health force in India. Established in 2006, it has 5 institutes around the country and provides cutting edge research and policy leadership to public and private sectors.
Apollo Hospital Group has set the standard for world class medicine in India since its founding 27 years ago. India’s initial leader in telemedicine and an experienced provider of call centers, it will offer those services and its medical expertise as the Initiative’s hospital partner. It is helping sponsor the 1000 Days Initiative through the Apollo Foundation. Apollo has recently begun the construction of 250 hospitals in tier 3 and 4 cities under its Apollo Reach program. In addition to taking the lead on medical direction, professional training, common telemedicine and call center systems, Apollo will also be one of our implementation partners, providing the wellness centers, health workers, and clean water services for a “for pay” model.
Ashoka has been leading the global social entrepreneurial sector for the 30 years since its founding and has nearly 600 Fellows working in health fields around the world. It also recently collaborated with General Electric and Boerhinger Ingelheim to support promising health innovations through global competitions. In addition, Ashoka’s Health for All program incubated Healthpoint Services which provides (from a “Healthpoint” facility) clean water, a clinic, diagnostics, and a pharmacy, backed up by a strong ICT system and telemedicine links to urban doctors. It has received both an Indian Sankalp Award for Best Emerging Enterprise and a Saving Lives at Birth Grand Challenge Award in 2011. Healthpoint will be one of our implementation partners.
The Harvard School of Public Health is a global leader in international health and brings unmatched research capacity to the Initiative. It will support PHFI in the monitoring and evaluation effort. Its work will be directed by the School’s immediate past Dean and the current Chairman of its Department of Global Health.
Thought Leadership and Governance Structure
The Initiative will be run by an Executive Committee (established by the Founding Parties), and managed by an Initiative Director, supported by appropriate staff and consultants. The Director will report to the Executive Committee. We will also establish a first-in-class thought leadership advisory council and a program of global experts for project support and integration of best practices. The structure will be as follows:
Executive Committee
Each founding party has a representative on this committee, which has overall responsibility. It hires the Initiative Director who manages the day to day activities of the Initiative.
Coordinating Committee
This is a broader committee of all those stakeholders with significant participation in the Initiative. All major participants in the trials will have a seat on the Initiative Coordinating Committee, which will meet regularly and be managed by the Initiative Director.
Expert Committees
We will recruit, staff, and support the following working expert committees of trial participants:
(a) Health and Wellness
(b) Information and communications technologies
(c) Training and public education
(d) Research
(e) Economics, business models and outcomes
Each expert committee will have a matching advisory committee recruited from global experts (including representation from Ashoka Fellows) and managed by PHFI to provide input, validation, education, and dissemination of their results. This will help us benefit from the successes and/or failures from around the world, while contributing our own experiences.
The Initiative staff will liaise with the government, private sector, non-governmental organizations and civil society on promoting, tracking and consolidating transformational health and wellness projects using modern ICTs in India. The staff will undertake coordination, education and advocacy with various international and local stakeholders as needed.
Leadership Committee
A diverse, broadly representative group of high level professionals will be recruited to provide intellectual leadership and input, for which the field trials will be a live experiment. Supported by program staff, it will write and adopt an overall Strategy for Change and revise it as needed.
[1] It is beyond the scope of this Initiative to reform the food supply chain and to change eating habits. We believe demand for both will be generated by seeing the results of nutrient repleteness.
[2] The system will be designed to connect to India’s new electronic identification initiative when it is ready for that.
[3] This is a program in a number of districts registering basic data on pregnancies and births using feature cell phones.
[4] Dimagi’s CommCare software is an excellent foundation for use by health workers. We will build on it by, for example, adding nutrition components and checklists that are being developed by Atul Gawande’s team and WHO.